
Doing something is a good start. But it’s not enough.
As evaluators we deal with all sorts of programs and activities that were launched out of a need to do something. Programs that keep on doing something, or something else, or something ineffective, or something effective, or something counterproductive, or something amazing, or nothing.
And it’s easy to come in and say, “well, why are you doing that?” or “what are you trying to accomplish?” That’s one of our jobs right? As an outsider, or quasi outsider, it’s not all that hard to ask these existential questions.
But what about the stuff that “we” do? Our work?
Not our methods, those are really just us doing things. What are we for?
EEI seeks to shift the evaluation paradigm so that it becomes a tool of and for equity and one that embraces the complexity of the age in which we live.
An Interview with Jara Dean-Coffey, Founder, Luminare Group

Seizing Momentum and Resisting Fatigue
Do you feel it?
The news cycle slowly shifting away.
Back to the usual.
We have never been more aware of the appalling events that occur around the world every day. But in the face of so much horror, is there a danger that we become numb to the headlines – and does it matter if we do?
Elisa Gabbert – Is compassion fatigue inevitable in an age of 24-hour news?
I was listening to Sam Sander’s fantastic podcast, It’s been a minute. One question came up when he was speaking with his guest Candace Carty-Williams on the Black Lives Matter protests the UK. It was the why now question.
Would these protests be happening at this scale if so many people across the globe were not stuck inside their houses? Because things are different, are we less likely to let the monotony of everyday work take our attention away from important issues like normalized systems of white supremacy?

I worry about the overwhelm that seems to be a major component of our modern world.
Understanding that there is a problem and that I am part of that problem is a step. The compelling desire to do something, and following through, is another step. But to keep things moving forward, we have to counter the systemic racism with systemic anti-racism. We have to contribute to change that is bigger than any one of us.
Not just because channeling our efforts into changing the system brings more potential. But because failing to channel our efforts can quickly lead to fatigue.
Despite the predicted prevalence of CF, the literature also suggests that compassion fatigue can be mitigated through activities that promote resilience such as: self-awareness, self-care, and mindfulness training.
Tara Tucker, Maryse Bouvette, Shauna Daly, and Pamela Grassau – Finding the sweet spot: Developing, implementing and evaluating a burn out and compassion fatigue intervention for third year medical trainees
Don’t get me wrong, this is not a call for inaction. We’re in a moment, there’s momentum, we need to leverage that momentum.
Just doing things is a great start, but is rarely ever a great long term solution.
Health Inequity

Today, Du Bois’ observation still stands true, as communities of color continue to experience higher rates of premature death and chronic disease compared to Whites, due to an interplay of social and economic factors, many grounded in the legacy of institutional racism and discrimination.
Shenae Samuels-Staple, PhD, MPH – The State of COVID-19 in Florida and South Florida: An Early Look at Disparities in Outcomes?
I’ve been working on the next module for my free dataviz for anti-racism course. It should be live sometime in the next week. I’ll send a message to everyone who is enrolled when it’s up.
The first module focuses on localizing police arrest data. The second module will dive into basic infographic design using special education data.
But given current COVID-19 trends, I thought I would take a little space today to run through uncovering inequity in public health data.
First things first, there is strong evidence of inequity within the COVID-19 data.
But it might not be easy to decipher in the numbers you see…
Data gets collected, analyzed, and reported in all sorts of ways. It varies across countries, states, and localities. But by and large, number of cases and number of deaths are common metrics.
In most states, this data is also further broken down by race and ethnicity. The CDC also has a report that shows the incomplete aggregate data at the national level.

You could look at this data and say, whoa, look at the White People numbers. They represent 39.4% of the deaths but only 16.7% of the cases…
But we are also talking about a group of people that represent 60% of the US population. A lot of the COVID data we have on cases is pretty suspect, so comparing deaths to the overall population is likely to give a more reliable view.

Given the incompleteness of the national data, let’s zoom down to the state level. And since general population data is often missing from datasets, let’s take a look at the overall population distribution first.
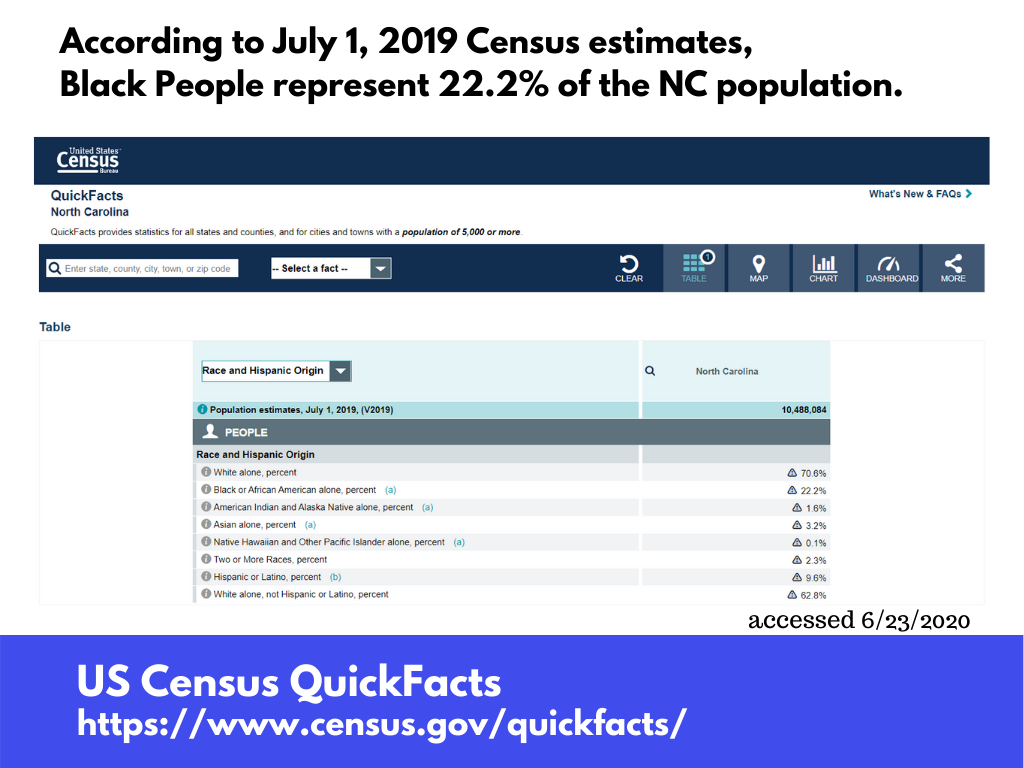
State data varies. But for health data I almost always start from the state’s health department. On NC’s site I found a page with the breakdown. And it was already in a format that made comparing cases and deaths pretty easy.

But as was mentioned before, let’s assume the death data is more reliable. So…
In North Carolina, Black People represent 22% of the population but 34% of the COVID-19 deaths. White People represent 71% of the population and 59% of the deaths.
This is the trend that seems almost universal across all sorts of data sources and fields. When something is bad, it’s usually worse for Black People than it is for White People. And the data reflects that.
So what about COVID-19 testing…
So after months and months, it’s still hard to trust the data we have on cases of COVID-19.
But like all things COVID, it’s harder to trust the case data in some states more than others. Johns Hopkins has a nice little visualization that compares all the states on their testing efforts. Let’s pull out a few.
So we start with number of tests. That number is then normalized to the population (making it so much easier to compare!). We also see the percent positive.
A combination of a high percent positive rate mixed with a low tests per 1,000 is a bit scary. It suggests under testing, which is also likely masking bigger numbers of cases.
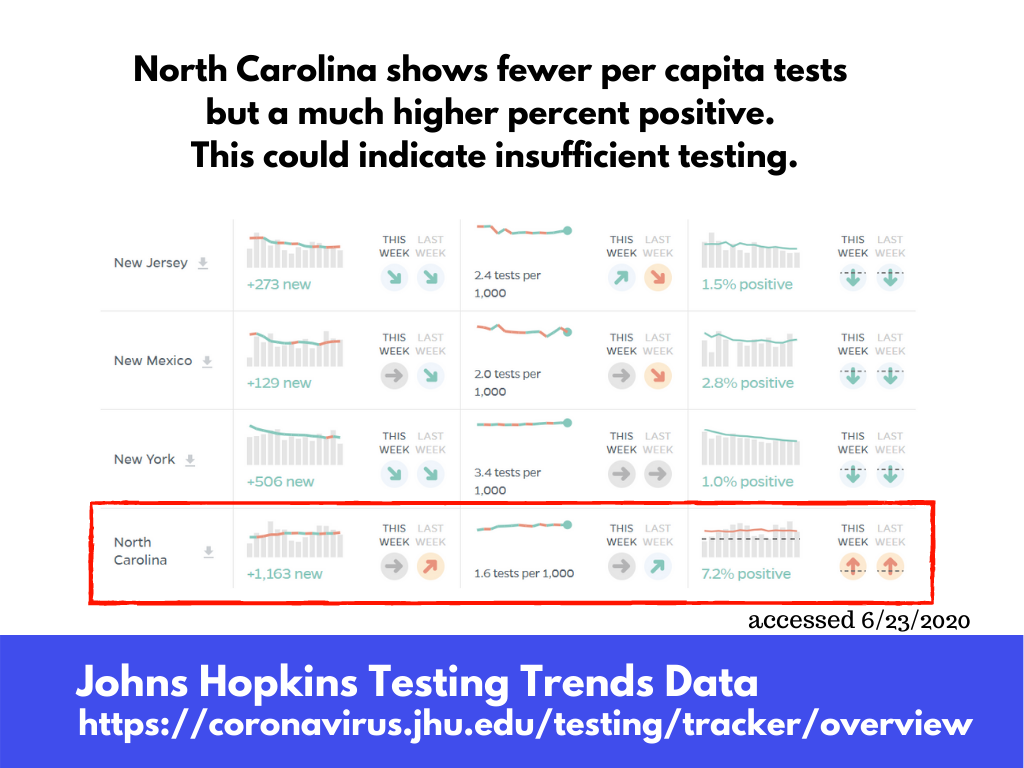
Two other southern states, Florida and Georgia, are also showing low testing rates and higher percent positive. Simultaneously, we’re still seeing pretty large spikes in cases for each of these states.

If only we could see how this testing slow down is impacting BIPOC communities.
But this data is not being shared…
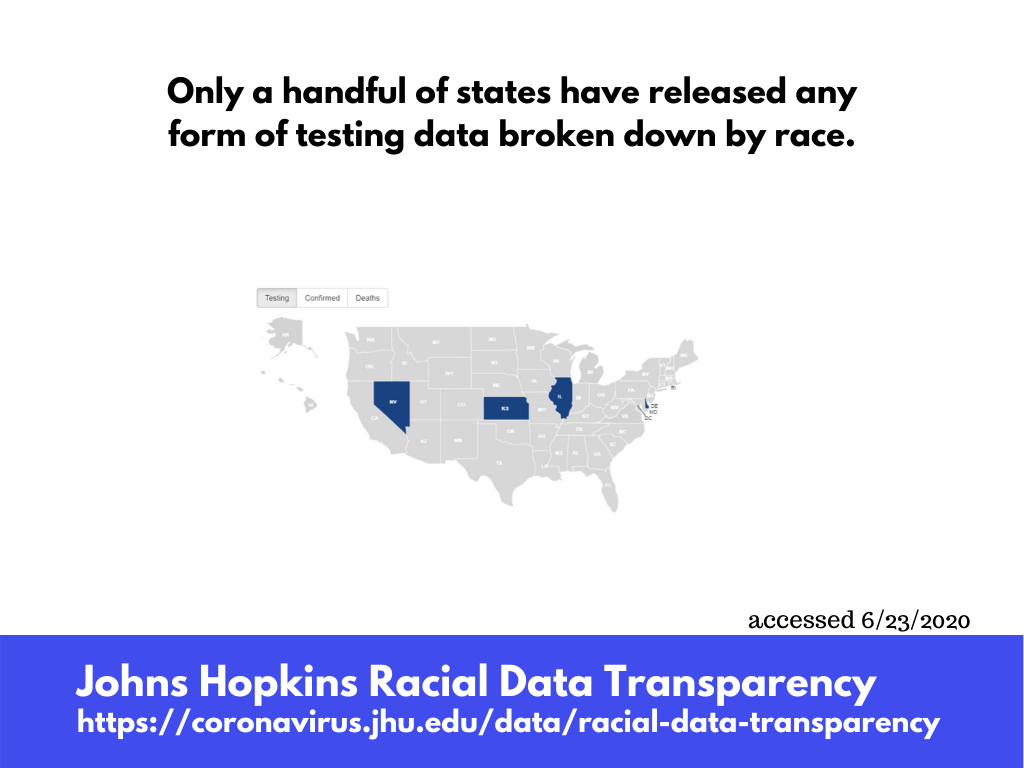
Having that data could help inform local efforts in combating the spread. But there is nothing to say that having testing data broken down by race will alleviate disproportional negative outcomes.
But it is distressing to think that the most reliable way to currently monitor the inequities relies on death rates.
It’s hard to properly drive a car when you close your eyes.
June 24, 1PM Eastern (10AM Pacific) Eval Central UnWebinar
I hope you can join us for this week’s Eval Central UnWebinar.
Special Guest: Mary Davis
This week’s seed topic: What do Public Health evaluators do?
Public health is a big, inclusive tent with evaluators from many disciplines and backgrounds. From her more than 25 years of experience, Mary will discuss the many roles that evaluators have in public health including preparedness–preparing for, responding to, and learning from pandemics and disasters.